By — Chetan Sarda, Zixuan Zhu, Yinong Yao, Randeep Singh
Final ROC curve on held-out test set — Random Forest, ROC AUC 0.801
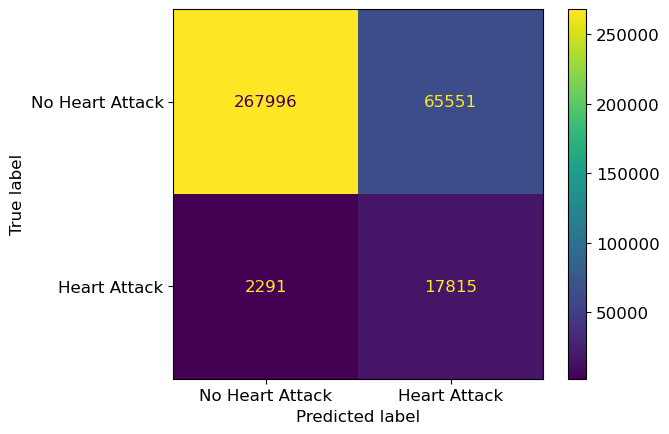
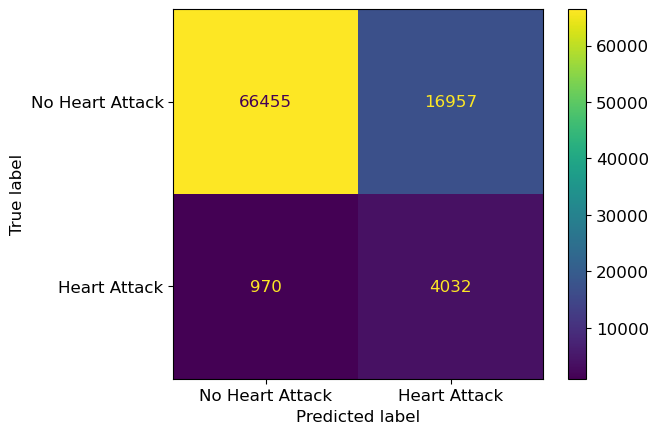
Final confusion matrix
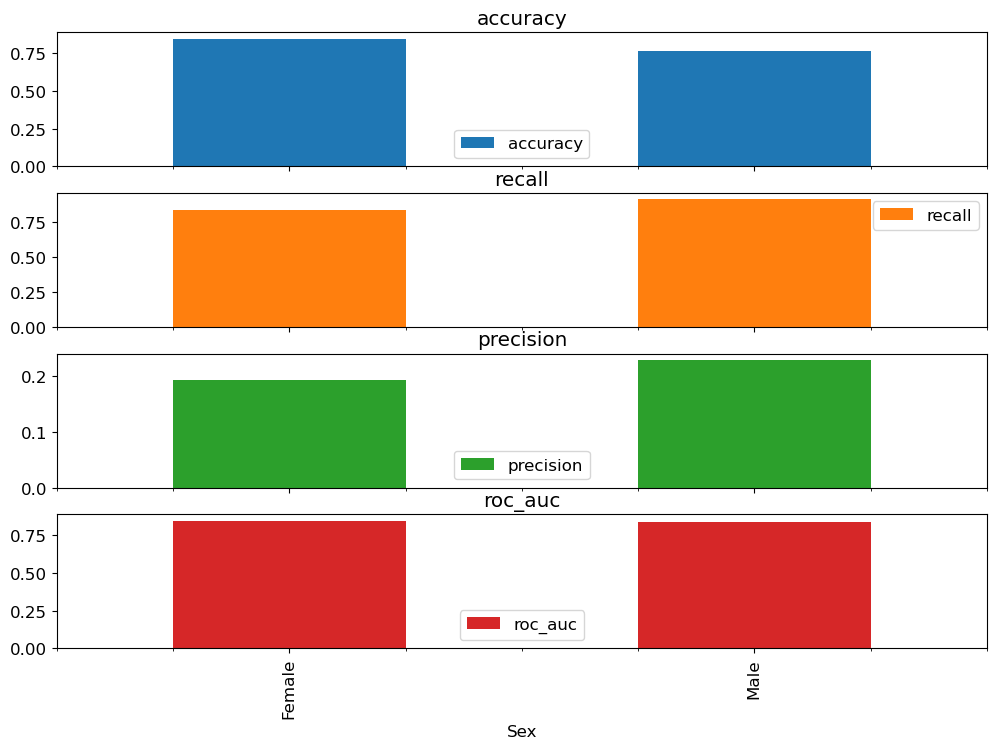
Fairness metrics by sex
This project came out of my MBAN capstone. We were handed a fictional client — Star City General Hospital — and told to build something that would actually help a hospital operate better. Most of my team gravitated toward churn or marketing-style problems; I pushed for heart disease because the public-health numbers were striking and the imbalanced-classification problem looked like a meaningful technical challenge.
The CDC figures are stark. Heart disease is the leading cause of death in the US — one person every 33 seconds. Roughly 47% of Americans have at least one of the three primary risk factors (high blood pressure, high cholesterol, smoking). Then you add diabetes, obesity (high BMI), low physical activity, excessive alcohol — and the list of people who should be flagged in a preventative-care program is enormous. The NHLBI's Framingham work has been pointing at obesity, sedentary lifestyle, and smoking as the dominant levers for decades. None of this is new. What's new-ish is that a hospital now has the data infrastructure to actually act on it at the individual-patient level instead of relying on population-level guidance.
Personally, I wanted to use this project to learn a few specific things:
sklearn Pipeline + ColumnTransformer setup that doesn't leak between train/test folds. I'd been burned by fit-on-everything mistakes before.